Restoring HopeFighting the Opioid Crisis in Buffalo

Tagline Meet Ben Francis Subtitle
Tagline Meet Ben Francis Subtitle

Ben Francis was a high school senior when his insides
betrayed him.
Ben says he was one of those “straight-edge”
kids. He’d avoided drugs and alcohol through his teens,
and in his spare time, played soccer and hung out with
his friends. He was a promising artist and aspiring art
teacher; photography, in particular, inspired him. His
life seemed to be following a trajectory familiar to
most of the kids who attended his large high school in
suburban Western New York, just outside of Buffalo.
But
after one high school soccer injury and three refills of
Vicodin—a powerful prescription opioid—Ben was teetering
on the edge of a new world. “I knew I liked the
feeling,” he says. Although, when the prescriptions ran
out, he says he “figured that was over.”
It wasn’t over, as Ben found ways to buy more
pills and, subsequently, heroin—anything that would
induce in his body the same sensations brought on by the
Vicodin. While taking classes at SUNY Potsdam, every
cent he earned went toward feeding his addiction, toward
calming the beast inside of him. “I would go so far as
to jump in the car at 5 a.m. with some friends and go to
the closest place to buy anything like that.”
“It became my life.”— Ben Francis

Ben Francis' descent
Ben Francis' descent

Ben managed to make it through a few weeks of classes
during his first semester of sophomore year at Potsdam.
Then he started disappearing for days and eventually
dropped out. Ben planned to come back the following
fall, but he never did. His descent continued.
What’s
misunderstood about addiction, Ben says, is that no one
wants to be that way. No one wants to feel that
way. Once the brain crosses that powerful
threshold—between recreational use and addiction—every
day is a struggle just to feel normal. Every day is a
brush with death, a race to find a dealer, a plan to
outsmart the cops and the people who love you.
At
this point, for Ben, it was no longer about getting
high. Rather, it was “about being able to function—about
being not sick.”

Ben's story is common
Ben's story is common
Ben continued to use. “I figured I was resigned
to that life until it killed me,” he says.
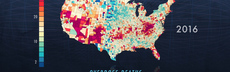
Ben’s story is common.According to the American Society of Addiction
medicine,20.5 million Americans age 12 or older had a substance
use disorder in 2015. Of those, 2 million used
prescription pain relievers and 591,000 used heroin.
Nearlya thirdof those who use heroin develop opioid addiction.
Easy access to drugs like heroin, fentanyl, and
even prescription medications like OxyContin has fueled
an epidemic of addiction—the deadliest in U.S. history.
Now, science is revealing how addiction affects the
brain, and experts are gathering evidence to determine
how we can best address our drug problem, from embracing
evidence-based treatments to rethinking public
policies.
As a whole, the U.S. is making some progress
toward untangling the web of factors fueling the opioid
crisis. But drug use is still on the rise. In 2017, it's
estimated thatmore than 72,000 Americans died from drug
overdoses,including illicit drugs and prescription opioids.
That’s more than triple the number of deaths that
occurred from drug overdoses in 2002. Life expectancy in
the U.S. is dropping because of this crisis.
“We have 4.5% of the world’s population in the
United States,” says Cheryll Moore, medical care
administrator at the Erie County Health Department in
Buffalo, NY. To put that in perspective, the U.S.
consumes 30% of the world’s opioid supply. “In the
United States of America, we do a quick fix and we got
in big trouble. We are getting out of it slowly.”

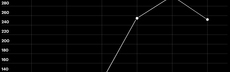
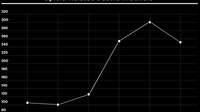
Opioid-Related Deaths in Buffalo
Opioid-Related Deaths in Buffalo
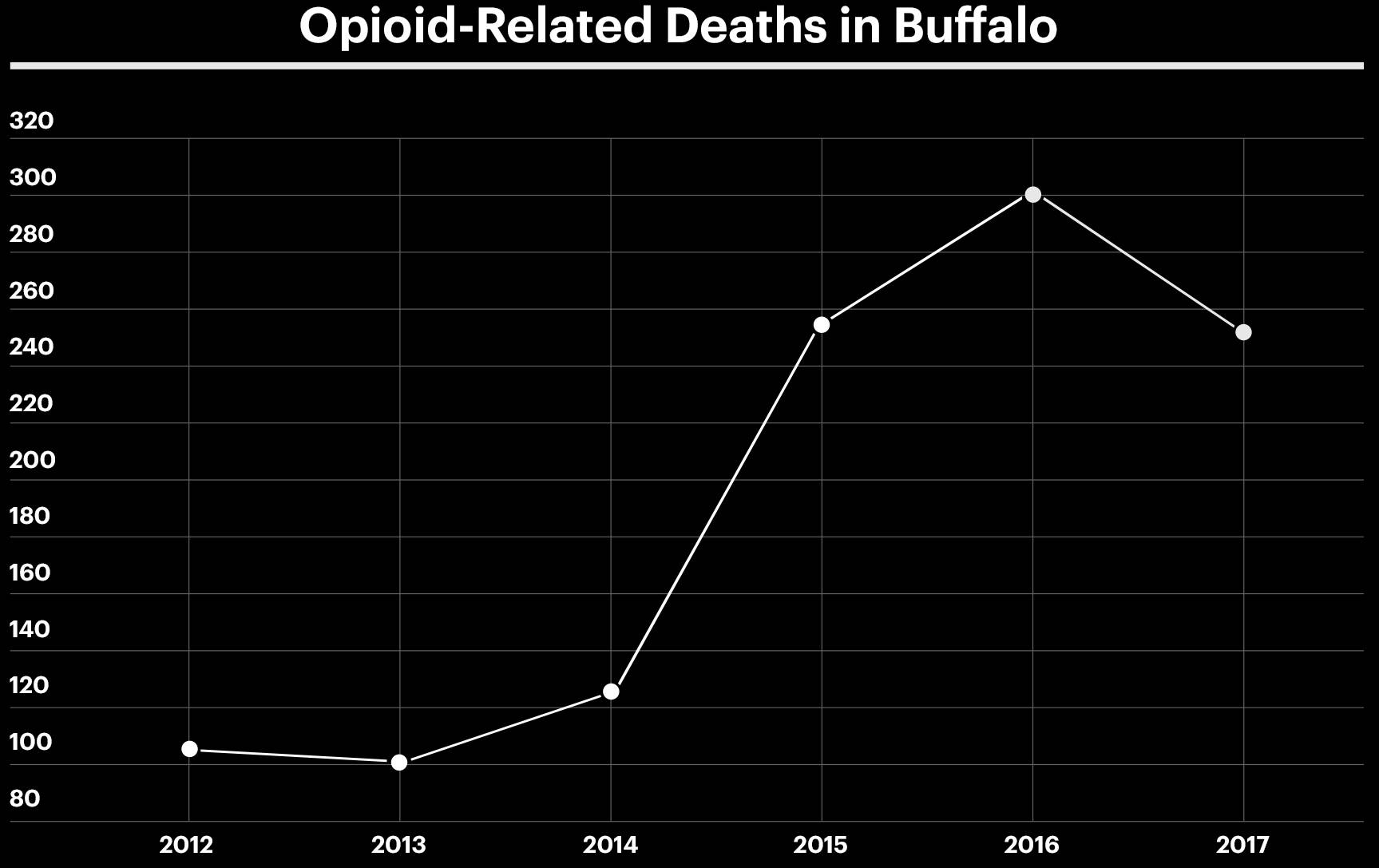
From 2009 to 2016, opioid overdose deaths doubled in
New York State.
However, a few areas have begun to see a
decrease in fatalities, including the city of Buffalo
and surrounding Erie County. What's behind the
decline?
New York's I-STOP law
Back in 2013, New York State’s I-STOP law was put into
effect, requiring prescribers to consult a Prescription
Monitoring Program Registry when writing prescriptions
for certain controlled substances. This provided
practitioners with secure access to prescription
histories for their patients. Officials and medical
experts in Buffalo thought this would help curb the
crisis.
It did not.

The Erie County Opiate Epidemic Task Force
The Erie County Opiate Epidemic Task Force

A new response was necessary in Buffalo.
Cheryll
Moore and her colleagues started the Erie County Opiate
Epidemic Task Force in 2017, which is made up of seven
working groups, including law enforcement, community
members, families affected by the crisis, medical
providers, health department officials, and more. “All
of the efforts of all of the work groups together, in
synergy, are starting to make inroads. We’re trying all
different programs—anything that we can,” Moore says.
“What’s working, we keep. What isn’t working, we get rid
of.”
This is how a lot of regions in the U.S.
are operating: on informed experimentation. Because the
opioid crisis is extremely complicated and varies county
by county, medical experts and policymakers are working
to get on the same page and make their process more
effective given limited resources.
One of the
task force’s programs that seems to be working is a new
response from police officers whenever they encounter an
overdose.
All hands on deck

Just outside Buffalo is the socioeconomically
diverse and historically blue-collar town of
Cheektowaga, the city’s second largest suburb. The
Cheektowaga Police Department’s attitude toward the
opioid crisis is all hands on deck. Officers are tightly
integrated with Cheryll Moore’s task force; officers
communicate with the health department and other parts
of the network directly after responding to an
overdose.
Lieutenant Brian Gould says when
his team arrives on the scene, the sight is a scary one.
The victim—sometimes collapsed on a bathroom floor in
the mall, sometimes slumped over against a
building—isn’t breathing. “They’re unresponsive,” Lt.
Gould says.
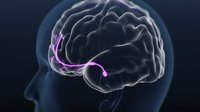
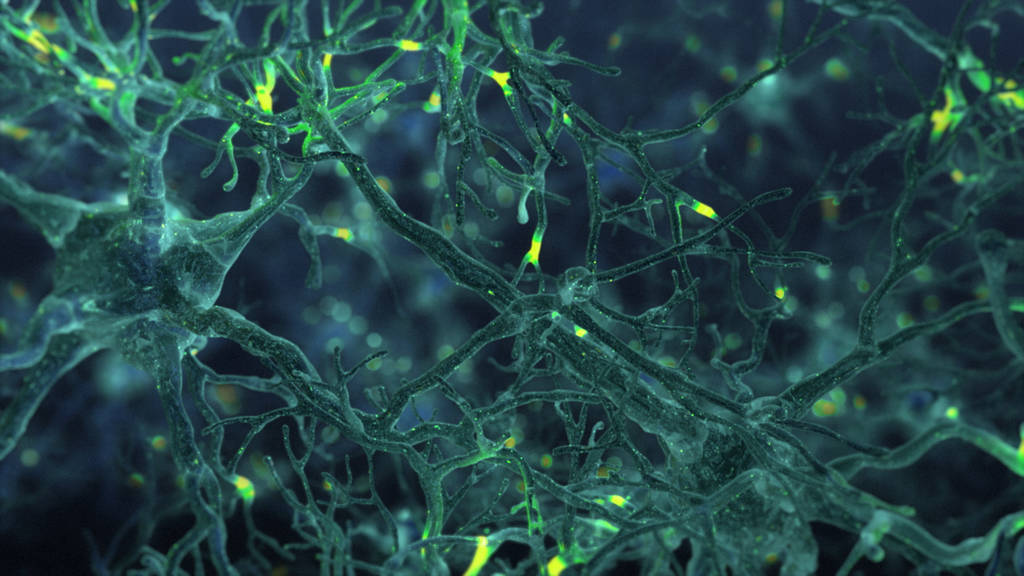
Take a look at the science behind opioid addiction:
Take a look at the science behind opioid addiction:
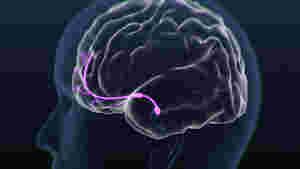


Breathing life back into the breathless

In the event of an overdose, a compound called naloxone
can revive someone on the brink of death. Sold under the
brand name Narcan and administered either by injection
or in the form of a nasal spray, naloxone can literally
breathe life back into the breathless.
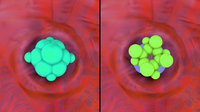
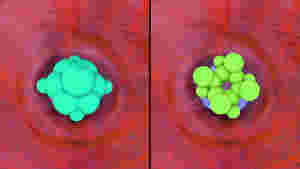
Naloxoneblocks the effects of opioidsby binding to opioid receptors—proteins that drive the
body’s response to these compounds by serving as docking
sites for opioid molecules. If there’s an opioid already
present on the receptor, naloxone kicks it off. Then,
when naloxone binds to the receptor, it blocks that
receptor’s activity but doesn’t activate it—meaning a
person can recover from his or her overdose.
Though
naloxone can bind to every kind of opioid receptor, it
has a particular affinity for mu opioid receptors. Mu
receptors can be bound by drugs like morphine, fentanyl,
and heroin. Their activity is responsible for the
euphoric, sedative, and pain-relieving effects
attributed to these drugs.
The exact way in which naloxone interacts with mu
receptors to displace opioids and restore breathing
remains unclear. The effectiveness of the drug, however,
is no mystery. Within minutes of receiving naloxone, an
overdose victim can regain consciousness and may even
experience sudden withdrawal symptoms.
A drug so powerful in reversing an overdose has
little to no effect on people without opioids in their
system. “You can’t mess it up,” Lt. Brian Gould says.
“If you administer naloxone to somebody who’s not having
an overdose situation, it has no negative effects. They
end up with a wet nose—that’s all.”
In Cheektowaga, police officers are equipped with
Narcan nasal spray kits. This is unusual—the number of
police forces carrying Narcan is changing rapidly. But
records suggest that the majority of law enforcement
officials do not carry Narcan, though it’s extremely
effective in saving lives. Since law enforcement
officials are typically the first people on the scene
after an overdose, and because time is of the essence
when a person isn’t breathing, a police officer’s
ability to administer Narcan can be the difference
between life and death.

Kickstarting a process

In Cheektowaga, after a person has overdosed and received Narcan, his or her information is quickly entered intoODMAP,an app created by the Washington/Baltimore High Intensity Drug Trafficking Areas (HIDTA) program. This database is used in various ways across the country, but in Cheektowaga, it kickstarts a process: The officer enters certain data into ODMAP (for example, location of the overdose, how many doses of Narcan were administered, whether the overdose was fatal or not); then Moore’s team dispatches someone to connect with the individual.
YOUR LIFE WAS SAVED THIS TIME
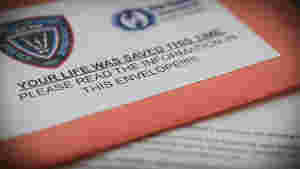
Meanwhile, law enforcement gives the person who has
overdosed a small but alarming package. It’s a bright
orange envelope with the words “YOUR LIFE WAS SAVED THIS
TIME” written in large bold letters.
“It’s
[an] envelope full of information on how to get help,”
Lt. Gould says. “We have a 24-hour opiate addiction
hotline—there’s a card in there for that. There’s
information on how to get naloxone. There’s information
on how to get people into treatment.” The orange packet
is a way for law enforcement to get this critical
information into the hands of overdose victims and their
loved ones.
“I scan this map three times a day.”— Cheryll Moore
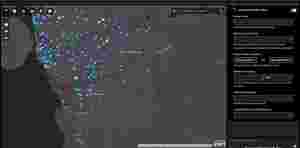
Every dot and diamond corresponds to an overdose.
The power of a peer

Cheryll Moore checks ODMAP in the morning, at lunch, and
at night. If there are any new overdoses, Moore
identifies the police department that was involved and
reaches out to their records clerk for a report. If the
person who has overdosed hasn’t called the health
department, then within 24 to 72 hours after the
overdose, Moore’s team deploys a peer—someone in
recovery who’s been trained to support those still
struggling with addiction—to talk to them and let them
know that they’re not alone. Most of the time, the
peer goes to the person’s home to see if they’re around;
as a backup plan, the peer will try reaching the person
by phone.
“Every case is unique,” Moore says.
“That’s the beauty of the peer asking someone, ‘What is
it that you’re looking for?’ The key is not what I want,
but what you want for you.”
The optimal goal
of this relationship is to connect the person with
long-term treatment. A peer also sits down with family
members to determine how best to support the
individual.
“We’ve interacted with 58 people
since September [2017], and since then, more than 60%
are still connected to treatment,” Moore says.
This
is all possible because of ODMAP, which connects people
to recovery options in near real time. Historically, the
health department received reports from law enforcement
about their use of Narcan, but it wasn’t necessarily
same-day information. These individuals are usually
“sick and tired of feeling sick and tired,” says Antonio
Estrada, one of the peers. They’re more open in that
vulnerable state to exploring treatment options, he
says. It’s important to note, though, that this window
of time is extremely fleeting; if the opportunity
passes, patients could end up in severe withdrawal and
go back to using.
As a peer, Estrada knows
what it’s like. He’s been in recovery for 18 years, and
can describe to overdose victims what the journey feels
like.

Medication-assisted treatment

Historically, diseases of addiction like opiate use
disorder were treated with abstinence-based programs
that included behavioral interventions, but no
prescription medications. However, without chemical
assistance to reduce the brain’s cravings, patients on
these types of treatments are muchmore prone to relapse,with failure rates estimated between 80 to 90%. Today,
so much of the opioid drug supply is tainted with
unpredictable amounts of potent fentanyl. Every time a
person uses, the risk of death is extremely high.
As
a result, more and more addiction specialists are
advocating for medication-assisted treatment or M.A.T.
This combines social and behavioral interventions with
drugs like methadone or buprenorphine that mimic the
body’s own pain relievers, reduce cravings, and help
regulate the production of dopamine.
"The treatment of choice"
"The treatment of choice"
For Dr. Paul Updike, the medical director for Substance
Use Services for the Catholic Health System in Buffalo,
NY, this approach is the “treatment of choice.” But he
notes that different treatments should be
“complementary, not exclusive of one another.”
There’s a growing consensus that emergency
departments should work aggressively to offer
medication-assisted treatment to every overdose victim
immediately—at the moment when they are most vulnerable
to relapse.According to the Recovery Research Institute,the window of time between referring a person to
treatment and his or her actual appointment, if too
long, could result in loss of motivation. Many addiction
specialists fear that after 24 to 72 hours, a patient
might already be in acute opioid withdrawal, and at
increased risk to use—and overdose—yet again.
“If
you have a diabetic patient whose blood pressure is too
high, and a few weeks later, the blood pressure got too
high again, you don't kick him out of the diabetic
clinic,” says Dr. John Aldis, an addiction medicine
specialist in the Eastern Panhandle of West Virginia.
“You welcome them back in, you get them back on
treatment, as often as is needed. And that isn't being
done in addiction medicine.”
At Massachusetts
General Hospital in Boston, people who have overdosed
are sent home with a prescription for a drug that
combines buprenorphine and naloxone (sold under the
brand name Suboxone). Unlike methadone, which is a
Schedule II drug and requires a DEA license to
prescribe, buprenorphine can be prescribed and given to
individuals right in a doctor’s office. According to the
Drug Addiction Treatment Act of 2000, doctors can
prescribe buprenorphine in a variety of settings
including community hospitals, health departments, and
prisons. On the other hand, methadone maintenance
treatment can only be performed in a Substance Abuse and
Mental Health Services Administration (SAMHSA)-certified
clinic.
In Western New York, many hospitals
are connected with Cheryll Moore’s task force. “Each
case is slightly different,” Moore says. In general,
overdose victims are transported to the local emergency
department after overdoses occur; at 13 of those
emergency departments, staff are trained and registered
to provide and prescribe Suboxone. Moore’s task force is
responsible for having trained 150 of those providers in
the past few years. Additionally, the individual is
given an appointment with a nearby long-term treatment
provider within two to seven days after the ER visit if
the individual so chooses to pursue long-term care.
“We currently have a network of 27
community-based substance use disorder providers that
have allocated more than 60 slots weekly for immediate
appointments and continuation of medication-assisted
treatment,” Moore says. This is necessary because the
initial prescription from the ED is only valid for a
week—then the patient is advised to follow through with
the arranged long-term treatment. If a client is
uninsured, the task force has set up a process with a
local Congressional Budget Office to accept donations to
pay for the first week of medication for the
individual.
This means that there are
essentially two paths for a person who has overdosed in
Buffalo: If a person enters an M.A.T.-participating
emergency room, he or she can find long-term care
immediately. If the person overdoses in Cheektowaga, he
or she might still receive the same treatment at the ER
(if that particular hospital has Suboxone providers),
but that person will also have received the orange
packet from law enforcement containing information about
peer support and M.A.T.
Until all emergency
rooms can provide Suboxone or methadone on demand,
community providers are doing the best they can to
engage people in treatment. In Buffalo, the task force
and peer system seem to be making a difference.
At
the Catholic Health System Methadone Clinic, the first
of its kind in Buffalo, Dr. Updike is focusing on making
sure people with opiate use disorder are stabilized with
medication-assisted treatment so they can get back on
track.
“When patients aren’t having to deal
with the demand of their addiction every day, then
things change dramatically,” he says. “There’s
concurrent care here—a counselor, nursing
staff…medication is an important piece of the treatment,
though.”
In general, medication-assisted
treatment works because opiate use disorder is a
chronic, life-threatening illness characterized by
changes in the brain. According to Dr. Updike, these
changes drive the stigmatizing behaviors often
associated with addiction—like criminality and
joblessness—and medication is necessary for a successful
recovery. “If we don't address that underlying problem,
then patients will struggle,” he explains.
This is how methadone and Suboxone work in the brain.

A work in progress

Many communities across the country have all but
neglected their opiate-dependent populations.
Others—those with sufficient resources—are trying to
construct ideal pathways and permanent solutions.
Ultimately, experts say that the best way forward is to
make sure all emergency departments are equipped with
on-demand methadone and Suboxone.
“We need
just as many spots open for addiction medicine as we
have for diabetic medicine or any other chronic,
relapsing, and potentially fatal disease,” Dr. John
Aldis says.
Given their limited resources,
Buffalo officials are devising an ambitious plan that
remains a work in progress.
"We have a long road ahead of us"
"We have a long road ahead of us"
Cheryll Moore knows there’s more work to be done. “We
have a long road ahead of us,” she says. “It’s going to
take a long time to get out.” In October 2018, Erie
Countyreceivedtwo grants from the Bureau of Justice Assistance for a
total of $1.8 million to fight the opioid epidemic.
Moore says that over the next three years, one million
will fund an Opioid Mortality Review Board to help shape
future public health practices and policies related to
opioid addiction. The remaining funds will be used to
develop a peer support unit for people suffering from
opiate use disorder and who are in the Erie County
probation system.
Additionally, Erie County
received $3.2 million of funding from SAMHSA and the New
York Department of Health to increase peer services,
increase access to naloxone, and provide training to
first responders in the eight counties of Western New
York over the next four years.
Working out
the kinks in systems like Buffalo’s will require taking
a hard look at the delicate time frame between an
overdose and a person’s next use of opioids. Dr. John
Aldis says that medications with a long half-life (that
is, medications that remain in the bloodstream for a
longer period of time) are the most promising, and that
medical care providers need to administer the first dose
of methadone or Suboxone once a person is in withdrawal
and after the effects of other opioids in the system
have subsided. Before that, these medications can make a
person very sick.
And once initiated, many
people are able to hold down a job, avoid street crime
and violence, and reduce exposure to HIV due to
injections only because they’re taking methadone or
Suboxone. Treatment, while a sacrifice, is much better
than its opposite.
More than anything, the
stigma around addiction needs to erode, says Dr.
Aldis.


Credits
Credits
Senior Writer: Allison Eck
Senior Digital Producer: Ari Daniel
Director of Photography: Arlo
Perez
Deputy Executive Producer: Julia
Cort
Production Assistance: Tim De Chant,
Nafisa Syed, Vincent Pham
Animator: Ekin
Akalin
Designers: Amelia Leason and Ken
Kimball
Developers: Hilary Emmons, Tim
Kinnel, Carl Lindberg
Additional Photography: Stephen McCarthy and Rob Lyall
Associate Researcher: Robin Kazmier
Producer/writer/director of NOVA Addiction:
Sarah Holt
Scientific Advisor: John Aldis,
MD
Digital Managing Producer: Kristine
Allington
Additional Footage: Shutterstock,
Getty, Freesound
Special thanks to everyone
in Buffalo we spoke with.
Watch NOVA's filmAddictionwhere you'll also find a set of resource links.
©
WGBH Educational Foundation 2018
#AddictionCrisisPBS