The Mental Health Crisis in North Carolina’s Emergency Rooms
May 16, 2023
Share
In partnership with:
Listen to the story:
Your browser does not support the audio element.
For the past month, WFAE has been examining North Carolina’s broken mental health system, especially as it affects people in the criminal justice system.
This week, we start to look at the impact this system has on others, like children who wait for weeks or months in hospital emergency departments because there’s simply no place for them to go. And people who head to emergency rooms in crisis, only to find the average wait for a state psychiatric hospital is more than two weeks.
The emergency room is supposed to be the place to go in a medical crisis. It’s not supposed to be a place to live for days or weeks. But that’s what’s been happening for many North Carolinians in the midst of a mental health crisis. They need a psychiatric hospital bed, but they can’t get one. The problem is so common there’s a name for it: boarding.
On any given day this January, an average of 350 North Carolinians waited in emergency rooms even after they needed a hospital bed, state data shows. They boarded in ERs because no psychiatric beds were available — either in a state hospital or a nonprofit or for-profit hospital, such as Atrium or Novant.
Seventeen-year-old Alexis Klunk knows what that’s like. She’s boarded multiple times, said her mom, Crystal Klunk. Alexis struggles with PTSD and suicidal feelings.
“When you were 10, that was the first time you had to go,” Crystal told her daughter recently. “Dad and I would not leave you because there were adults, and Dad and I slept on the floor.”
“That’s probably why I was scared,” Alexis said. “Because I remember when I was experiencing it, I was short. That’s how I know I was a little kid.”

Crystal said she’s tried to avoid bringing her daughter to the ER. One time, she said she and her husband took over a week off work so they could watch Alexis at home until a bed became available.
But sometimes, she said, she’s had no choice. She remembers one of those visits when Alexis spent several days in the ER. For part of that time, she remembers, she waited in a room with others in crisis, including adults.
Read and listen to the series: FRACTURED
“In that waiting room, there was, I remember, a lady across from us,” Crystal said. “She was coming off of drugs. Because I remember you being, like, ‘What’s wrong with her?’”
Alexis said, “The lady, she was rocking back and forth. She was sweating like crazy. She looked like she was about to die.”
ERs Aren’t Designed for In-Depth Mental Health Care
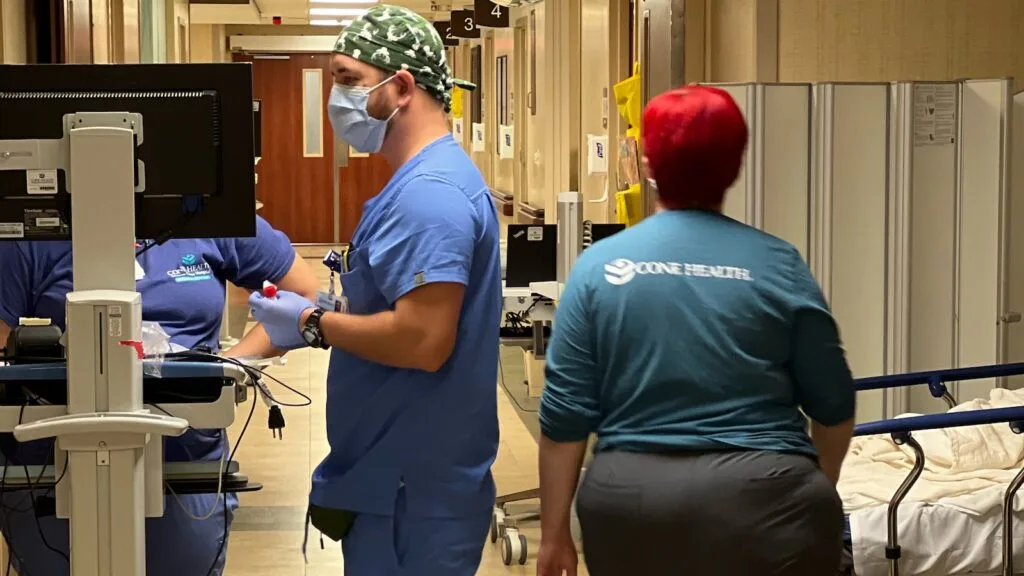
Hospital emergency rooms are set up to quickly stabilize patients in crisis, then move them out. They’re not good environments for those experiencing a mental health crisis, says Dr. Kevin Steinl. He heads emergency medicine for Cone Health, which operates hospitals and outpatient care in central North Carolina. Alexis Klunk has never stayed in one of his ERs, but Steinl says even the best emergency departments aren’t good environments for those grappling with a mental health crisis.
“The ER is a bright, loud, noisy, sometimes very chaotic, always changing environment that’s on 24/7, 365. And just imagine yourself being in that setting for, you know, one week, one, month, six months,” Steinl said.
It’s especially bad for kids, he said. They don’t have access to schooling, or the ability to play outside. And it’s not the place to get the mental health treatment many may need, Steinl said. If someone has gone off their medication, ER doctors can restart it. But many patients need more.

“What gets a patient or person through crisis – meds might be one part, but it might be therapy, counseling, giving them skills and tools to avoid crisis or to empower themselves in some way, “ Steinl said. “Those are all things that typically aren’t happening on a consistent basis in an emergency department setting.”
Adults with good insurance and easily-treated problems can get a bed in a community hospital in one day, Steinl said. But uninsured and hard-to-manage patients wait much longer.
Read more: Fractured: The Wait Inmates With Mental Illness Endure Because They’re Too Sick For Trial
And there are too few juvenile and geriatric beds. So if a child like Alexis or an elderly person needs a bed, “that’s kind of a road to nowhere because literally there was next to nowhere that we could find to accept those folks,” Steinl said.
“They can remain on that list in the same position for three months, four months, with no movement,” Steinl said.
Cone has a team of social workers to help patients find placements, but it’s still difficult, Steinl said. It’s even harder for families. Sometimes they just can’t cope anymore. In extreme cases, he’s seen children or elderly people with mental health problems abandoned in the ER. Sometimes families drop them off — and don’t come back.
“It’s almost a ‘Tag. You’re it.’ phenomenon. ‘We are tired. We can’t do this any longer. Good luck, it’s now your problem,’” Steinl said.
Some children are abandoned in the ER for weeks. A state health department dashboard shows that 27 kids sat in emergency rooms in the first three months of this year. Eleven of them were in the custody of county social service departments. A representative for Cone Health said those children board for an average of 66 days in their ERs.
Boarding isn’t good for patients — and it’s a problem for the community, too. Behavioral health patients who board typically take up 20% of Cone’s ER beds, Steinl said. That eats into the emergency department’s capacity to quickly treat everyone who needs care. A typical ER visit takes three to four hours, on average, he said. So when ER staff can’t find a placement for someone?
“They might stay in our department in some cases for upwards of six months in time. If that happens, we lose the ability to care for hundreds of patients through that one bed,” Steinl said.
Why North Carolina Has a Boarding Problem
Boarding wasn’t a problem when Steinl first became an ER doctor 25 years ago. But that was before North Carolina overhauled its mental health system, cutting in half the number of state psychiatric beds and converting outpatient care into a privatized system which relied on Medicaid. A lot of people got left out.
Today there are 1.2 million uninsured North Carolinians, according to Kody Kinsley, the Secretary of the North Carolina Department of Health and Human Services. They include many with serious mental illnesses.
Some end up on the streets, some end up in jails. And many wait in emergency rooms. ERs used to be the canaries in the coal mine — the first sign of the brokenness of the state’s mental health system. But not anymore, Kinsley said.
“Frankly, we’re way past canaries in a coal mine,” Kinsley said. “I mean, this has been a crisis for a long time, and our health care system is feeling it more acutely now than ever because of the staffing challenges they’re facing. But, it didn’t just come on the scene.”
Those with the most complicated mental health problems might need to be in a state psychiatric hospital. But it’s hard to get one of those beds. Staffing shortages mean that only 600 of the state’s 900 state beds are operating. And many of those are filled with people who won’t be leaving any time soon.
One-third are filled with inmates who need care just to be able to stand trial. Four in ten of the remaining beds are filled with patients who are ready for discharge, NCDHHS data shows. It can take months before they’re discharged because there’s no place for them to go. There’s a shortage of community care for those with mental health needs.
The result is that boarding patients who need a bed in a state psych hospital wait in ERs an average of 16 days.
Read more: Life Sentence on the Installment Plan
Community hospitals — whether nonprofit or for-profit — are a different story. It turns out there actually are enough adult psych beds there. But, on average, only 80% are in operation at any given time, state data shows. Staffing shortages contribute, but Kinsley said hospitals often won’t take patients who either lack insurance – or whose insurance won’t pay enough.
“Part of that calculus is finances, that either those people don’t have insurance or they’re underinsured or the rates aren’t sufficient for them to maintain the staff necessary for the complex level of care they need to provide,” Kinsley said.
And if you’re waiting in the ER for residential care, like a group home, you’ll have a tough time getting that too, says Nicholle Karim, of the North Carolina Healthcare Association, which represents the state’s community hospitals. She agrees the problem is finances.
North Carolina’s Medicaid program pays significantly less for mental health care than other states do. And national data shows the state’s private insurers pay less than insurance companies in most other states too.
Without adequate pay, a lot of therapists, nurses and aides, who are essential to residential care, decide to leave the mental health field.
“Until they feel like they can make a living taking insurance or being on Medicaid, we will continue to see what we’re seeing, where almost half of all therapists and psychiatrists don’t take any insurance and just do self-pay,” Karim said.
And that means there are fewer people to staff residential care. So there’s less available.
“In some instances, we have to send kids out of state because we don’t have it here. And that is – that should be our metric for change. We shouldn’t have to send people out of state.”
One hundred ninety kids with behavioral health problems were sent to out-of-state psychiatric residential treatment facilities in the first three months of this year, according to state data.
In March, the North Carolina legislature voted to expand Medicaid. It won’t go into effect until the state enacts a budget. Then, an estimated 600,000 North Carolinians will be eligible for coverage. Secretary Kinsley said that will have a small but immediate effect on emergency room boarding because community hospitals with empty psych beds will now have paying customers.

Right now, he said, there are 130 empty beds with staff who can immediately begin serving patients. Kinsley said they can be turned on “in a flash.”
Kinsley also hopes the legislature will approve a plan to spend $1 billion on mental health using federal expansion dollars. If the legislature OKs it, there would be money to build out a crisis support system to divert people from emergency rooms. It would also increase those Medicaid reimbursement rates to try to grow the mental health workforce.
Dr. Steinl of Cone Health is hopeful too, but he worries that even if all that money is approved, it won’t make a difference for the growing number of people stuck in his emergency rooms.
With a standalone psychiatric hospital, another psychiatric ward, and a new geriatric mental health unit, Cone has a greater ability to place patients than most emergency rooms. But Steinl says that hasn’t been enough to stem the problem.
“What’s happened in the last five years, the growth of this problem is not a linear growth. It’s exponential,” Steinl said. “There are days when fully 90-95% of our ER beds are occupied by boarding patients.”
And it means long waits for others who need emergency care.
WFAE’s Mona Dougani contributed to this report.
This story is part of a collaboration with WFAE through FRONTLINE’s Local Journalism Initiative, which is funded by the John S. and James L. Knight Foundation and the Corporation for Public Broadcasting.
Additional reporting on this story:
The Story Behind Fractured, a WFAE Investigation — by Dana Miller Ervin
Fractured: Frequently Asked Questions — by Dana Miller Ervin
Methodology: Data Collection — by Robert Benincasa, Mona Dougani, Julia Ingram
Why Data About Capacity to Proceed is Important — by Neil Gowensmith
The National Picture on Wait Times for Restoration — by Susan McMahon
Mental Health Care in North Carolina Jails — by David L. Rosen
WFAE Reporter, WFAE
Email:
DErvin@wfae.orgRelated Documentaries

Latest Documentaries












Related Stories

Fractured
Related Stories
Fractured
Explore
Policies
Teacher Center
![]()
Jon and Jo Ann Hagler on behalf of the Jon L. Hagler Foundation
Corey David Sauer
Koo and Patricia Yuen
FRONTLINE is a registered trademark of WGBH Educational Foundation. Web Site Copyright ©1995-2025 WGBH Educational Foundation. PBS is a 501(c)(3) not-for-profit organization.
Funding for FRONTLINE is provided through the support of PBS viewers and by the Corporation for Public Broadcasting, with major support from Ford Foundation, and The Fialkow Family Foundation. Additional funding is provided the Abrams Foundation, Park Foundation, John D. and Catherine T. MacArthur Foundation, Heising-Simons Foundation, and the FRONTLINE Trust, with major support from Jon and Jo Ann Hagler on behalf of the Jon L. Hagler Foundation, and Corey David Sauer, and additional support from Koo and Patricia Yuen. FRONTLINE is a registered trademark of WGBH Educational Foundation. Web Site Copyright ©1995-2026 WGBH Educational Foundation. PBS is a 501(c)(3) not-for-profit organization.